 |
| Click on image to enlarge. Source |
The General Accounting Office reported last week that Medicare Advantage (MA) plans, the private health plans that care for one in five Medicare beneficiaries, receive a windfall because of their effectiveness at coding member illnesses. This is a quandary – capitation for Medicare members is only reasonable if there is careful risk adjustment. The Deficit Reduction Act of 2005 required risk adjustment to be phased in by 2010.
Physicians in Medicare Advantage plans have a strong incentive to use coding to maximize the apparent illness of their patients. Physicians in traditional Medicare are paid only based on services provided, so they have little incentive to aggressively code diagnoses. As a result, the apparent severity of illness of Medicare beneficiaries who have chosen the private plans has increased dramatically faster than the severity of illness of Medicare beneficiaries on traditional Medicare.
It’s actually a bit worse than that. The Medicare Advantage plans put an enormous amount of energy into coaxing their participating physicians to aggressively code comorbidities during 2007-2009. Here’s an example of how much it’s worth. The Medicare payment goes up by 16% for diabetics, but goes up by over 50% for those who also have evidence of kidney or blood vessel involvement. Mild diabetic kidney disease is quite common, but was rarely coded before risk adjustment. Now, physicians participating in Medicare Advantage know that they must use the ICD9 code for diabetes with renal manifestations (250.4) at least every other year, or they will not get the maximum Medicare budget.
Here are Medicare risk adjustment factors associated with diabetes. (See HCC_Coefficients_2009-2012) Note that multiple comorbidities allow an additional upward adjustment, further encouraging more aggressive coding.
 |
| Click on image to enlarge. Source |
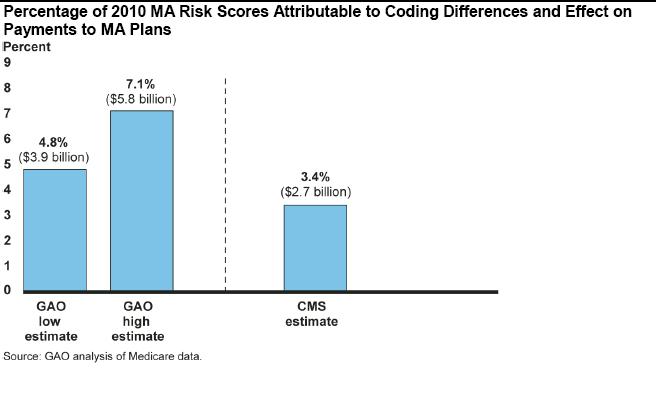
CMS has been aware of this for some time, and as a result the agency has lowered all reimbursement to MA plans by 3.4% ($2.7 billion). However, the GAO analysis suggests that the increased costs associated with aggressive coding are between 4.8% ($3.9 billion) and 7.1% ($5.8 billion).
Across-the-board cuts to reimbursement to counteract differential coding aggressiveness means that all physicians associated with MA plans have to work even harder to be the most aggressive at coding complications. If they merely code the same way as physicians participating in traditional Medicare, their reimbursement will fall each year.
The conclusion from a recent FTC analysis of gaming of risk adjustment:
Before risk adjustment, MA plans had an incentive to enroll individuals who were low cost, both along dimensions that will later be included in the formula and those that will not. Because risk adjustment increases payments for individuals with the conditions included in the formula and decreases payments for those with few or no conditions, risk adjustment lowers the payments MA plans would receive for these individuals, as they were selected to have low risk scores.
But in response to the new incentives created by risk adjustment, selection patterns into
MA change. After risk adjustment, MA plans have less incentive to avoid individuals with
the conditions included in the formula but have a greater return to enroll individuals who
have low costs conditional on their risk score. Indeed, relative to individuals who remain in FFS…MA enrollees' risk scores increase after risk adjustment, but their costs conditional on their risk score fall so much that, if anything, MA enrollees have lower total costs after risk adjustment.
There is no easy answer to this problem. MA plans would seek the lowest risk Medicare beneficiaries if there were no risk adjustment. However, they will seek to maximize the proceeds of risk adjustment when it is in place, and seek to select low-risk beneficiaries based on measures that are not included in the risk adjustment. At a minimum, CMS should rebalance the risk adjustment “code creep” factor each year. Further, CMS should consider applying this factor differentially to groups that have a high level of apparent “code creep.” It’s possible that this could be done using ceilings on annual adjustments by group, exempting groups with very small or much-changed membership.
The sad fact is that it’s easier to code aggressively than perform more effective medical management on the Medicare population.













